People who experience food insecurity or loneliness are much more likely to develop chronic pain after surgery, according to new research presented at the ANESTHESIOLOGY® 2025 annual meeting.
Chronic pain – lasting three months or…

People who experience food insecurity or loneliness are much more likely to develop chronic pain after surgery, according to new research presented at the ANESTHESIOLOGY® 2025 annual meeting.
Chronic pain – lasting three months or…
V-pattern strabismus is one of the most common alphabetic patterns.1 It involves a more convergent (or less divergent) horizontal deviation in downgaze than in upgaze and becomes clinically significant when vertical incomitance exceeds 15 prism diopters (Δ).2
Undoubtedly, in most cases, the V-pattern is associated with the presence of inferior oblique muscles overaction (IOOA), which leads not only to vertical and horizontal deviations but also to excyclodeviation. Excyclotorsion resulting from inferior oblique overaction is thought to contribute to the development of V-pattern strabismus by inducing extorsional displacement of the globes, thereby increasing horizontal divergence in downgaze.3–5
Most V-patterns are, however, congenital or develop early in life, allowing suppression or anomalous retinal correspondence to prevent subjective awareness of excyclodeviation. Despite this, objective excyclotorsion in patients with V-pattern strabismus can be observed in fundus photographs, as shown in Figure 1.
|
Figure 1 A fundus photograph demonstrating bilateral ocular excyclotorsion in patient with bilateral inferior oblique overaction (authors own material).
|
Objective cyclotorsion is the measurable rotation of the eye around its visual axis, assessed using landmarks like the fovea and optic disc. The disc-foveal angle (DFA) is commonly measured via fundus photography, scanning laser ophthalmoscopy, or automated software, with studies comparing their accuracy and clinical utility.6–9 In 2021 our team developed Cyclocheck, a web-based diagnostic tool (freely available at www.cyclocheck.com) for measuring objective cyclotorsion in both clinical and research settings and proved it to be a repeatable and reliable method for office based DFA assessment.10,11 Figure 2 shows a screenshot of the Cyclocheck software interface.
 |
Figure 2 Cyclocheck software interface.
|
Bilateral graded recession of the inferior oblique muscles effectively corrects V-pattern strabismus across varying degrees of their overaction.12,13 It allows tailoring the surgical dosage according to IOOA severity and extent of V pattern, reducing both vertical and horizontal incomitance.14–16 It has also been proven to have prominent incyclorotating effect in patients with various types of strabismus associated with IOOA.17 However, to the best of our knowledge, no study to date has evaluated the effect of bilateral inferior oblique graded recession on objective cyclotorsion asymmetry, specifically comparing the impact of symmetric and asymmetric surgeries.
This study aims to evaluate changes in objective cyclotorsion using Cyclocheck following bilateral graded inferior oblique recession in patients with V-pattern strabismus and inferior oblique overaction. It also aims to investigate the impact of symmetric and asymmetric surgeries on cyclotorsion asymmetry between the eyes.
This retrospective study analyzed consecutive cases of patients presenting (eso/exo) V-pattern strabismus (≥15 prism diopters difference in measurement between upgaze and downgaze) with IOOA who underwent bilateral inferior oblique muscle graded recession, with or without concurrent horizontal rectus surgery. Eligible participants demonstrated binocular vision and had no history of strabismus surgeries, including procedures on other vertically acting muscles. Informed consent was obtained from each participant. The recorded data included age, gender and the amount of V-pattern, defined as the difference between down- and upgaze. It also covered the amount of inferior oblique (IO) muscle recession in millimeters for each eye separately, the total recession for both eyes combined, and pre- and post-operative objective cyclotorsion measured by Cyclocheck using fundus photographs. Digital fundus photographs of both eyes of all study subjects were obtained using a DRS nonmydriatic fundus camera (CenterVue DRS Automatic Retinal Camera, Welch Allyn). All measurements were made before and 3 months following the surgery. Photographs were taken under binocular viewing conditions while the subject looked at an internal fixation target. A chin and forehead rest with side marks were used as a guide to ensure proper head position. The disc-foveal angle was calculated using a web-based diagnostic tool for assessing objective cyclotorsion named Cyclocheck.
The inferior oblique recession was classified as “symmetrical” when the same degree of recession was performed on both eyes, provided the vertical deviation in the primary position was less than 5 prism diopters. If hypertropia ranged from 5 to 10 prism diopters, the recession in the more hypertropic eye was increased by 2 mm; for 10 to 15 prism diopters, by 4 mm; and for 15 or more prism diopters, by 6 mm. The amount of inferior oblique muscle recession was determined based on the severity of overelevation in adduction: +1 IOOA corresponded to 8 mm of recession, +2 IOOA to 10 mm, +3 IOOA to 12 mm, and +4 IOOA to 14 mm.
All procedures performed in studies involving human participants conformed to all local laws and were by the ethical standards of the Bioethical Committee of the Medical University in Lodz, Poland and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Bioethical Committee of the Medical University in Lodz, Poland (RNN/260/23/KE).
Comparisons were made using paired t-test and Wilcoxon signed-rank test. Normality of data distribution was assessed using the Shapiro–Wilk test. Paired t-tests were used for normally distributed variables, while non-normally distributed variables were analyzed using the Wilcoxon signed-rank test. Correlations between the variables were evaluated using the Pearson correlation coefficient (r). A Fisher’s z-test was used to examine the difference between two correlation coefficients. Statistical analysis was conducted using Python (Python Software Foundation, Netherlands). A p-value of ≤ 0.05 was considered statistically significant.
A total of 50 patients (100 eyes) were included in the study. The gender distribution was comparable, with 26 females and 24 males. The mean age was 10.46 years. V-pattern esotropia was observed in 22 patients (44%), and exotropia in 28 patients (56%). All the patients enrolled in the study underwent uneventful bilateral inferior oblique muscle graded recession of 8, 10, 12 and 14 mm as detailed in the methodology section. The procedure was symmetrical in 21 cases and asymmetrical in 29 cases (22 by 2 mm, 5 by 4 mm and 2 by 6 mm). The mean inferior oblique recession in millimeters was 10.92±1.81 in the right eye and 10.92±1.94 in the left eye, with the bilateral absolute amount of 21.84±3.04. The amount of V-pattern decreased significantly in all cases, but a residual V-pattern was observed in 4 cases (8%) – 5-10 PD of vertical incomitance in 3 cases and 25PD in one case (the patient had preoperative V-pattern of 50PD). Clinical characteristics of the study participants are presented in Table 1.
 |
Table 1 Clinical Characteristics of the Study Participants
|
A positive correlation was observed between the preoperative amount of V-pattern and preoperative absolute objective cyclotorsion (r=0.36, p=0.0093). This was no more valid postoperatively when absolute objective cyclotorsion had a light negative correlation with remnant V-pattern (r= −0.09, p=0.0001). A positive correlation was observed between the amount of IO recession and the change in absolute objective cyclotorsion (r = 0.46, p = 0.00), as shown in Figure 3. The mean reduction of objective cyclotorsion was 2.52° of cyclotorsion/ per 2 mm of recessed inferior oblique muscle. As shown in Figure 4, the total change of absolute objective cyclotorsion was moderately correlated with the reduction of the V-pattern (r=0.38, p=0.0032).
 |
Figure 3 The correlation between the amount of inferior oblique recession and change in absolute objective cyclotorsion.
|
 |
Figure 4 The correlation between the total change in absolute objective cyclotorsion and the reduction of the V-pattern.
|
A linear relationship was observed between the amount of inferior oblique recession in each eye separately and the change in objective cyclotorsion of the respective eye (right eye: r=0.37, p=0.0083; left eye: r=0.37, p=0.0087). The correlations were less evident than the one for both eyes, but they did not differ significantly (Fisher’s z-test 0.72 p=0.47). There was a positive correlation between the amount of preoperative objective cyclotorsion and the surgically induced change in objective cyclotorsion for each separate eye (Wilcoxon signed-rank test z= 6.452, p= <0.0001, Paired t test t= 5.1309, df= 54, p= <0.0001).
We also examined symmetric and asymmetric surgeries to assess their impact on cyclotorsion asymmetry between the eyes. Overall, the mean cyclotorsion asymmetry was significantly lower postoperatively (preoperative: 5.50°±3.40° vs postoperative: 4.00°±3.00°, p<0.001). However, this was independent of whether the surgery was symmetric or asymmetric. The influence on the amount of cyclotorsion asymmetry was similar in both groups (RE/LE difference: symmetric group 1.55°±4.15° and asymmetric group 1.47°±3.30°; p=0.938).
Inferior oblique overaction (IOOA) and associated V-pattern strabismus present significant challenges in strabismus management, often requiring surgical intervention to restore ocular alignment and minimize torsional deviations. Our study contributes to the growing body of evidence supporting graded inferior oblique recession as an effective approach for reducing both objective cyclotorsion and V-pattern deviation.14,17,18
Multiple studies have investigated the effect of inferior oblique muscle weakening procedures on ocular torsion. As early as 1986, Kushner, in his research evaluating cyclotorsional effects, noted that weakening the inferior oblique or tightening the superior oblique resulted in long-term incyclorotation (clockwise for right eyes and counterclockwise for left eyes) of the axis of astigmatism by approximately 10°.19 Sharma et al20 compared Fink’s recession with modified Elliot and Nankin’s anteropositioning, both of which resulted in a comparable degree of intorsional shift (+2.5° and +4.7°, respectively), with no statistically significant difference between the two techniques. The mean preoperative extorsion was 9.8° in patients undergoing Fink’s recession and 11.4° in those undergoing modified Elliot and Nankin’s anteropositioning. A study by Farid et al21 evaluated the effect of inferior oblique anterior transposition (IOAT) on fundus torsion and detected significant decrease from 12.67±8.13° preoperatively to 3.40±5.06° postoperatively. Sethi et al17 compared various inferior-oblique weakening procedures achieving mean reduction in excyclotorsion 3.65° in group treated with inferior oblique recession.
The mean preoperative objective cyclotorsion in our study was 13.48°±6.36° in the right eye and 11.50°±6.71° in the left eye, consistent with the expected presence of excyclotorsion in patients with V-pattern strabismus and inferior oblique overaction.22–24 Notably, the mean disc-foveal angle (DFA) reported by Sethi et al17 for patients undergoing inferior oblique weakening for primary or secondary inferior oblique overaction was 11.52°±7.15°, a value closely aligning with our findings, further supporting the reproducibility of these measurements in similar patient populations. Similarly, a study by Lee et al18 investigating objective excyclotorsion following graded inferior oblique recession in patients with primary and secondary inferior oblique overaction (IOOA) reported a mean preoperative torsional angle of 13.25°±6.74° in patients with primary IOOA and 16.91°±7.57° in those with secondary IOOA.
A moderate positive correlation was found between the preoperative amount of V-pattern and absolute objective cyclotorsion (r=0.36, p=0.0093). However, postoperatively, this relationship was no longer observed, as absolute objective cyclotorsion showed a slight negative correlation with the remaining V-pattern (r= −0.09, p=0.0001), showing that V-pattern improvement is largely independent of the degree of torsional correction. A possible explanation for this result is that the surgical correction of the V-pattern strabismus and inferior oblique overaction disrupted the preoperative relationship between the magnitude of the V-pattern and objective cyclotorsion. Postoperatively, as the V-pattern was significantly reduced, the remaining variation in cyclotorsion may have been influenced by other factors, such as individual differences in muscle elasticity, neural adaptation, or residual oblique muscle function. Additionally, the slight negative correlation could suggest a compensatory mechanism, where some patients with minimal residual V-pattern exhibited greater postoperative cyclotorsion adjustments due to neural adaptation or changes in extraocular muscle dynamics. These mechanisms were examined in the study by Schworm et al, which analyzes the underlying factors contributing to the well-documented long-term postoperative subjective cyclotorsional changes.25
Following surgery, our study population showed a significant reduction in objective cyclotorsion (right eye: 5.99°±4.50°; left eye: 8.39°±3.82°), ultimately aligning closely with the levels observed in normal subjects. The average disc-foveal angle, as reported in the literature and confirmed by our previous research, typically ranges between 5° and 7.5°.7,11,26–29
The average excyclotorsion reduction observed in our study population was 2.52° for every 2 mm of inferior oblique muscle recession. These results are consistent with Harada et al30 estimated a 1° change for every 1 mm of recessed inferior oblique muscle. Lee et al18 reported Lee et al18 reported a statistically significant change in cyclorotation, but did not establish a correlation between the degree of recession and the change in cyclorotation, making it impossible to directly relate our results to his findings.
Moreover, we observed a positive correlation between the amount of inferior oblique recession and the change in absolute objective cyclotorsion (r=0.46, p=0.00), indicating that greater recession generally resulted in a more significant reduction in cyclotorsion. A similar observation was made by Sethi et al.17 A linear relationship was also detected when analyzing each eye separately, with similar correlation coefficients for the right (r=0.37, p=0.0083) and left eye (r=0.37, p=0.0087). Although these correlations were slightly weaker when considering both eyes together, the difference was not statistically significant (Fisher’s z-test 0.72, p=0.47). This suggests that while inferior oblique recession influences cyclotorsion at the individual eye level, the overall binocular effect remains consistent, reinforcing the effectiveness of this procedure in managing torsional misalignment.
Interestingly, we found a positive correlation between preoperative objective cyclotorsion and the change in postoperative objective cyclotorsion in each eye. This suggests that the eye with greater preoperative excyclotorsion undergoes a greater change in objective cyclotorsion following surgery. Our results align with those of Sethi et al17 who suggested that, at the pooled data level, this correlation might partly stem from the graded approach to inferior oblique weakening. In this approach, the choice of surgical procedure depends on the degree of inferior oblique overaction and the V pattern, with more powerful weakening procedures typically performed in eyes with greater baseline excyclotorsion. Additionally, they propose a possible “self-adjusting” mechanism in inferior oblique weakening procedures, in which the degree of preoperative excyclotorsion influences postoperative changes in excyclotorsion, regardless of the final anatomical position of the inferior oblique – an idea that warrants further examination.
We observed a significant reduction in the mean V-pattern, decreasing from 18.62Δ±9.77Δ to 2.26Δ±5.76Δ(p<0.0001). Sethi et al17 also reported a significant reduction in V-pattern, from 19.20Δ±6.31Δ to 6.45Δ±4.05Δ. However, these values represent all procedures evaluated in their study (including inferior oblique recession, recession and anteropositioning, anterior transposition, and anterior and nasal transposition), making direct comparison with our results difficult.
The procedure demonstrated a high success rate, with complete resolution of the V-pattern in 46 cases included in our study, accounting for 92% of the study population. The total change of absolute objective cyclotorsion was moderately correlated with the reduction of the V-pattern (r=0.38, p=0.0032). Taken together, these results support the role of graded inferior oblique muscle recession as an effective surgical option for the management of V-pattern strabismus. As stated in the introduction, no study to date has assessed the effect of bilateral inferior oblique graded recession on cyclotorsion asymmetry, particularly in terms of comparing the impact of symmetric and asymmetric surgeries. Postoperatively, we observed a significant reduction in cyclotorsion asymmetry between the eyes. However, our analysis detected that this reduction occurred regardless of whether the surgery was performed symmetrically or asymmetrically. Both surgical approaches demonstrated a comparable impact on cyclotorsion asymmetry, with the RE/LE difference measuring 1.55°±4.15° in the symmetric group and 1.47°±3.30° in the asymmetric group (p=0.938).
A study by Yilmaz et al31 examined the effects of unilateral and bilateral inferior oblique myectomy (IOM) on fundus torsion in patients with primary and secondary IOOA. Their findings demonstrated that bilateral IOM significantly reduced both the mean disc-foveal angle (DFA) and DFA asymmetry between the eyes across all patient groups. However, due to the fact that with this procedure, the remaining muscle is released freely into the Tenon’s capsule, the exact location where the muscle will reattach is unpredictable and thus difficult to compare among patients. This is why, direct comparison of the above-mentioned study with our results is limited.
Undoubtedly, our findings suggest that the symmetry of the procedure is not a determining factor in postoperative cyclotorsion alignment. Instead, other factors may play a more significant role in the observed improvements, highlighting the need for further investigation.
Possible limitation of our study is the retrospective design of this study, which may have led to potential bias in establishing causation. Additionally, the follow-up period was limited to 3 months, which may not capture long-term changes in cyclotorsion; however, based on our clinical experience and previous observations, the effect appears to be long-lasting. The relatively small sample size without a formal power analysis may limit the reliability of subgroup findings. An additional limitation of this study is that concurrent horizontal rectus muscle surgery was performed in some patients, which may have acted as a confounding factor and influenced the postoperative changes in ocular alignment or cyclotorsion.
Graded inferior oblique muscle recession is an effective surgical technique for reducing objective cyclotorsion and V-pattern deviation. Our findings demonstrate a significant correlation between the total amount of muscle recession and the overall change in absolute cyclotorsion. However, changes in cyclotorsion of individual eyes were not reliably predicted by the amount of recession in each eye. Additionally, postoperative reduction in interocular cyclotorsional asymmetry occurred regardless of whether the surgery was performed symmetrically or asymmetrically.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
1. Zhu B, Wang X, Fu L, Yan J. Pattern strabismus in a tertiary hospital in Southern China: a retrospective review. Medicina. 2022;58(8):1018. doi:10.3390/medicina58081018
2. Saxena R, Dhiman R. Pattern strabismus. American academy of ophthalmology. Available from: https://www.aao.org/disease-review/pattern-strabismus.
3. Knapp P. Vertically incomitant horizontal strabismus, the so-called A and V syndromes. Trans Am Ophthalmol Soc. 1959;57:666.
4. Phillips PH, Hunter DG. Evaluation of ocular torsion and principles of management. In: Rosenbaum AL, Santiago AP, editors. Clinical Strabismus Management, Principles and Surgical Techniques. Philadelphia: WB Saunders; 1999:52–72.
5. Guyton DL. Ocular torsion: sensorimotor principles. Graefes Arch Clin Exp Ophthalmol. 1988;266(3):241–245. doi:10.1007/BF02181189
6. Jonas RA, Wang YX, Yang H, et al. Optic disc – fovea angle: the Beijing eye study. PLoS One. 2015;10(11):e0141771. doi:10.1371/journal.pone.0141771
7. Vélez Escolà L, Galán Terraza A, Lagrèze WA, et al. Disc-foveal angle and ocular counterrolling as a key in its interpretation. Arch Soc Esp Oftalmol. 2019;94(12):585–590. doi:10.1016/j.oftal.2019.05.019
8. Kanku MS, Sele S, Held U, et al. Cyclotorsion measurement on scanning laser ophthalmoscopy imaging compared with fundus photography in patients with fourth nerve palsy and healthy controls: cySLO-IV study. J Neuroophthalmol. 2012;41(4):e612–e618. doi:10.1097/WNO.0000000000000996
9. Jethani J, Dave P. A technique for standardizing disk foveal angle measurement. J AAPOS. 2015;19(1):77–78. doi:10.1016/j.jaapos.2014.08.015
10. Simiera J, Loba P. Cyclocheck: a new web-based software for the assessment of objective cyclodeviation. J AAPOS. 2017;21(4):305–308. doi:10.1016/j.jaapos.2017.02.009
11. Simiera J, Ordon AJ, Loba P. Objective cyclodeviation measurement in normal subjects by means of Cyclocheck® application. Eur J Ophthalmol. 2021;31(2):704–708. doi:10.1177/1120672120905312
12. Sokeer SH, Caldeira JA. V-pattern esotropia: a review; and a study of the outcome after bilateral recession of the inferior oblique muscle: a retrospective study of 78 consecutive patients. Binocul Vis Strabismus Q. 2023;18(1):35–48.
13. Caldeira JA. Some clinical characteristics of V-pattern exotropia and surgical outcome after bilateral recession of the inferior oblique muscle: a retrospective study of 22 consecutive patients and a comparison with V-pattern esotropia. Binocul Vis Strabismus Q. 2004;19(3):139–150.
14. Sokeer SH, Ali AL, Arafa ES, Awara AM, Shafik HM. Evaluation of graded recession of inferior oblique muscle for correction of different grades of V-pattern strabismus. BMC Ophthalmol. 2023;23(1):462. doi:10.1186/s12886-023-03210-x
15. Mostafa AM, Kassem RR. Comparative study of unilateral versus bilateral inferior oblique recession/anteriorization in unilateral inferior oblique overaction. Eur J Ophthalmol. 2017;28(3):272–278. doi:10.5301/ejo.5001062
16. Huang YT, Chen JJ-Y, Wu M-Y, et al. The effects of modified graded recession, anteriorization and myectomy of inferior oblique muscles on superior oblique muscle palsy. J Clin Med. 2021;10(19):4433. doi:10.3390/jcm10194433
17. Sethi A, Dhiman R, Mahalingam K, et al. Evaluation of change in objective cyclotorsion after various inferior oblique-weakening procedures. J AAPOS. 2023;27(6):345. doi:10.1016/j.jaapos.2023.08.016
18. Lee D, Kim WJ, Kim MM. Comparison of excyclotorsion following graded inferior oblique recession for primary versus secondary inferior oblique overaction. Int J Ophthalmol. 2020;13(8):1281–1286. doi:10.18240/ijo.2020.08.15
19. Kushner BJ. The effect of oblique muscle surgery on the axis of astigmatism. J Pediatr Ophthalmol Strabismus. 1986;23(6):277–280. doi:10.3928/0191-3913-19861101-05
20. Sharma P, Thanikachalam S, Kedar S, Bhola R. Evaluation of subjective and objective cyclodeviation following oblique muscle weakening procedures. Indian J Ophthalmol. 2008;56(1):39–43. doi:10.4103/0301-4738.37594
21. Farid MF, Sherin Bayoumy A, Seada M. Changes in fundus torsion following anterior transposition surgery of the inferior oblique muscle. BMFJ. 2023;40(surgical issue):55–67.
22. Cho SY, Lee SY, Lee CY. Clinical evaluation of excyclotorsion in patients with primary inferior oblique overaction. J Korean Ophthalmol Soc. 2012;53(9):1324–1329. doi:10.3341/jkos.2012.53.9.1324
23. Na KS, Lee SY, Lee YC. Ocular torsion in unilateral superior oblique palsy. J Korean Ophthalmol Soc. 2007;48(10):1388. doi:10.3341/jkos.2007.48.10.1388
24. Kushner BJ. A”, “V”, and other alphabet pattern strabismus. In: Taylor D, Hoyt CS, editors. Pediatric Ophthalmology and Strabismus.
25. Schworm HD, Eithoff S, Schaumberger M, Boergen KP. Investigations on subjective and objective cyclorotatory changes after inferior oblique muscle recession. Invest Ophthalmol Vis Sci. 1997;38(2):405–412.
26. Lengwiler F, Rappoport D, Jaggi GP, Landau K, Traber GL. Reliability of cyclotorsion measurements using scanning laser ophthalmoscopy imaging in healthy subjects: the CySLO study. Br J Ophthalmol. 2018;102(4):535–538. doi:10.1136/bjophthalmol-2017-310396
27. Williams TD, Wilkinson JM. Position of the fovea centralis with respect to the optic nerve head. Optom Vis Sci. 1992;69(5):369–377. doi:10.1097/00006324-199205000-00006
28. Bixenman WW, von Noorden GK. Apparent foveal displacement in normal subjects and in cyclotropia. Ophthalmology. 1982;89(1):58–62. doi:10.1016/S0161-6420(82)34862-9
29. Miyata M, Yoshikawa M, Ohtsuki H, et al. Age-related change and sex difference over 60s in disc-fovea angle in Japanese population: the Nagahama Study. Acta Ophthalmol. 2018;96(7):840–845. doi:10.1111/aos.13642
30. Harada M, Ito Y. Surgical correction of cyclotropia. Jpn J Ophthalmol. 1960;8:88–96.
31. Yilmaz OF, Oguz H. Evaluation of the effect of unilateral and bilateral inferior oblique myectomy on fundus torsion in primary and secondary inferior oblique overaction. North Clin Istanb. 2023;10(5):657–665. doi:10.14744/nci.2023.74875


Most children – including nearly 80% of infants – go without clear liquids before surgery for at least twice as long as guidelines recommend, according to an analysis of data on more than 70,000 children presented at the…

Northern lights (aurora borealis) illuminate the night sky over Vienna during a geomagnetic storm on May 11, 2024. (Photo by MAX SLOVENCIK/APA/AFP via Getty Images)
APA/AFP via Getty Images
Each Monday, I pick out North America’s celestial…
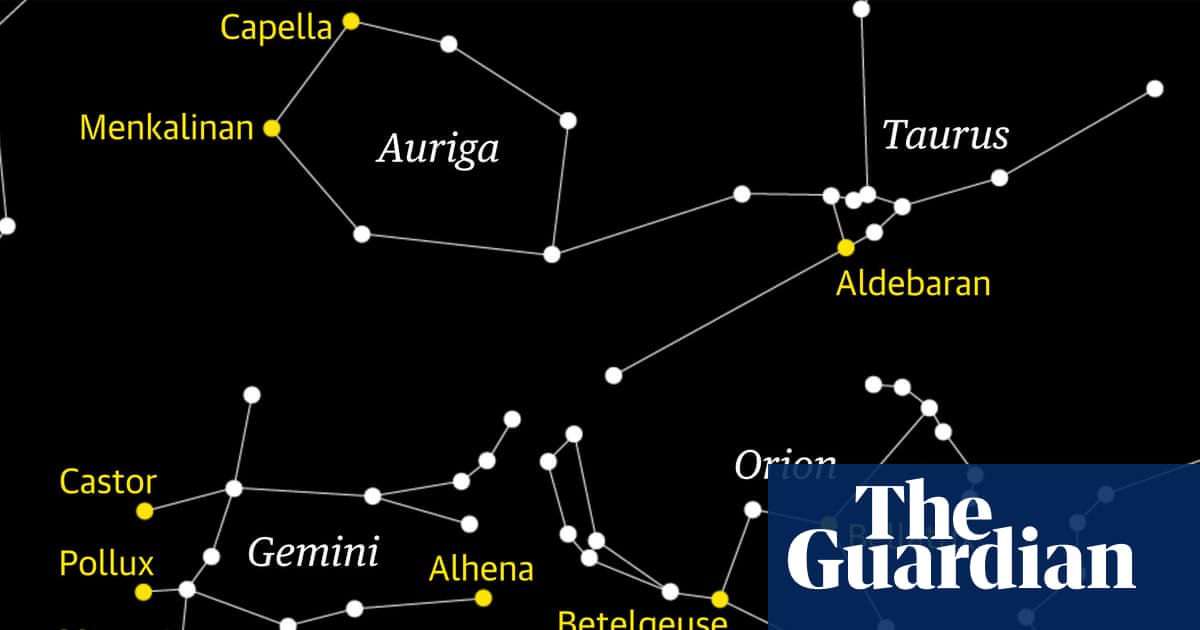
It is worth staying up for this pleasing view of the moon as it encounters Jupiter and the brightest stars of Gemini, the twins. The chart shows the view looking east from London at 00:30 BST in the very early morning of 14 October.
Gemini will…
Osteoarthritis (OA) is a primary cause of disability and chronic pain, impacting approximately 500 million people worldwide, with forecasts of almost one billion by 2050.1,2 OA considerably lowers the quality of life due to its characteristic progressive joint deterioration, pain, and loss of mobility. Though they provide short-term comfort, non-steroidal anti-inflammatory medicines (NSAIDs) and corticosteroids present significant gastrointestinal, cardiovascular, and renal hazards when used long-term.3,4 While effective for some, surgical interventions are invasive, costly, and not universally accessible.
These restrictions have fueled a rise in interest in integrative and alternative treatments. The monosodium iodoacetate (MIA) model has been a valuable instrument for reproducing important OA characteristics in preclinical research. Therefore, it is a promising avenue for assessing new, non-pharmacologic treatments.5,6 The GB34 acupoint, located near the fibular head, is often used for joint-related indications in both experimental and clinical settings. Evidence suggests that stimulation at GB34 can modulate inflammatory processes and promote cartilage preservation.7–9
Acupuncture has gained recognition for its affordability,10 safety,11,12 and effectiveness in managing musculoskeletal pain. The American College of Rheumatology conditionally recommends it for knee OA,13 with reviews supporting its pain-relieving and functional benefits.14–17 Acupuncture treatments such as Electroacupuncture (EA), bee venom acupuncture (BVA), and laser acupuncture (LA) differ in mechanism while sharing common targets. Although previous studies have noted the therapeutic benefits of LA, EA, and BVA in OA.18–23 This study is the first to directly compare these treatments under the same conditions. This direct comparison fills a critical gap in the literature, providing valuable insights for clinical decision-making in integrative pain management. The potential impact of these findings on the future of pain management is significant.
This study was approved by the Dongshin University Animal Committee (DSU-2024-07-04). All animal care and experiments were conducted under the Guide for the Care and Use of Laboratory Animals of the National Institutes of Health and Dongshin University Institutional Animal Care and Use Committee policies.
Forty-eight male Sprague-Dawley rats (8 weeks old, 240–280 g; SAMTAKO Korea) were housed under controlled conditions (22 ± 2°C, reversed 12-hour light/dark cycle) with ad libitum access to food and water.
Male rats were used to reduce differences in pain and inflammatory responses caused by sex hormones. This decision was based on previous research showing that pain from OA varies significantly with a rat’s age and sex.24
OA was induced via intra-articular injection of monosodium iodoacetate (MIA; Sigma-Aldrich, St. Louis, MO). MIA was dissolved in 30 μL of sterile saline at 1 mg. Under brief isoflurane anesthesia, the injection was administered into the medial side of the patellar ligament of both knees using a 19-gauge, 0.5-inch needle, ensuring the needle did not penetrate the cruciate ligaments. The control group received an equivalent volume of sterile saline. Post-injection, the limbs were gently massaged before returning the rats to their housing.
Rats were randomly assigned to six groups (n = 8 per group): Control (Con): No OA induction or treatment. OA: MIA-induced OA without treatment. Manual Acupuncture (MA): MIA-induced OA treated with manual acupuncture at GB34. Invasive Laser Acupuncture 830nm (830nm): MIA-induced OA treated with 830nm invasive laser acupuncture at GB34. Electroacupuncture (EA): MIA-induced OA treated with Electroacupuncture at GB34. Bee Venom Acupuncture (BVA): MIA-induced OA treated with bee venom acupuncture at GB34.
All acupuncture treatments commenced one-week post-MIA injection and were administered three times per week for four weeks.
Manual Acupuncture (MA): Sterile acupuncture needles (0.25 mm diameter, 13 mm length) were inserted bilaterally at GB34 to a depth of approximately 5 mm. Needles were manually stimulated with gentle twirling for 30 seconds every minute during a 3-minute session.
Invasive Laser Acupuncture 830nm: Using the Ellise device (Wontech Co. Ltd., Daejeon, Republic of Korea), an optic fiber-coupled laser diode was inserted into sterile acupuncture needles. The laser was set at 50Hz, 20mW, and applied for 3 minutes per session at GB34 on both legs to a depth of 5 mm.
Electroacupuncture (EA): Sterile stainless-steel acupuncture needles (0.25 mm diameter, 13 mm length) were inserted bilaterally at GB34 to a depth of approximately 5 mm. Electrical stimulation was applied using a constant current EA device, delivering alternating frequencies of 2/10 Hz at an intensity of 1 mA for 3 minutes per session.
Bee Venom Acupuncture (BVA): A 0.1 mL injection of bee venom solution (1.0 mg/mL) was administered subcutaneously at GB34 using a 30-gauge insulin syringe to a depth of approximately 5 mm.
Joint pain severity was assessed using the paw withdrawal threshold (PWT) test with manual von Frey filaments. Rats were acclimatized for 10 minutes in individual boxes. A filament with a bending force of 0.6 g was applied perpendicularly to the plantar surface of each hind paw until it bent slightly, and the response was recorded. If no response was observed, a filament with the next higher force was used; if a response occurred, the next lower force was applied. This up-down method continued until a pattern of responses allowed for calculating the 50% withdrawal threshold. Each paw was tested three times, with a 3-minute interval between tests. The mean values were used for statistical analysis. PWT assessments were conducted before MIA induction and weekly thereafter for four weeks.
Behavioral and structural outcomes were assessed up to 4 weeks post-MIA and treatment, a time window known to capture pain progression, early cartilage, and bone alterations in MIA-induced OA models.25,26
After the treatment period, the rats were euthanized using a carbon dioxide (CO2) gas chamber via a gradual-fill method, following the AVMA Guidelines for the Euthanasia of Animals (2020 Edition). This approach ensured a humane endpoint, minimizing pain and distress. The right knee joints were harvested, fixed in 4% paraformaldehyde, and subjected to micro-CT scanning using the Quantum GX2 imaging system. Data were analyzed using AccuCT™ software (PerkinElmer).
Following micro-CT scanning, knee joint tissues were decalcified in 0.5M ethylenediaminetetraacetic acid (EDTA, pH 8.0) for twentyone days, with the solution changed every two to three days. After decalcification, tissues were dehydrated through a graded ethanol series, cleared in xylene, and embedded in paraffin wax. Paraffin blocks were sectioned sagittally at nine μm thickness using a microtome. Safranin O/fast green staining was used to assess cartilage integrity. The severity of osteoarthritis was evaluated using the Osteoarthritis Research Society International (OARSI) scoring system and the Mankin score.
Data were analyzed using R software (version 4.3.2) and presented as mean ± standard deviation (SD). Data was assessed for normality using the Shapiro–Wilk test, and a parametric method was applied. Comparisons between groups were made using one-way analysis of variance (ANOVA) followed by Tukey’s post hoc test for multiple comparisons. A p-value < 0.05 was considered statistically significant.
Paw withdrawal thresholds (PWT) were monitored over time to assess acupuncture’s impact on mechanical allodynia. Before MIA-injection, all groups exhibited similar baseline PWTs (15.2±0.9g), confirming no pre-existing differences. One-week post-MIA induction, all groups showed a rapid and sustained reduction in PWT, confirming pain hypersensitivity (Figure 1A) while the control group remained stable Acupuncture-treated rats showed progressive recovery. By Week 2, EA and LA groups showed modest improvements (p < 0.05; p<0.01 vs OA) while MA and BVA groups did not show any significant improvement. From Week 3 onward, LA and EA exhibited further gains (p < 0.01), with all three modalities demonstrating significant pain reversal by the final week (LA: p < 0.001; EA: p < 0.01; MA: p < 0.05). Weekly comparisons revealed that LA maintained a significant reduction from week two onwards, EA was improved on week two and four and MA started showing improvement from week four (Figure 1B).
|
Figure 1 Changes in paw withdrawal threshold over 4 weeks across different treatment groups in MIA-induced OA rats. (A) Changes in paw withdrawal threshold over time. (B) PWT values for groups from Week_1 to Week_4; n=8 per group. Data are presented as the mean ±standard deviation; p<0.05, p <0.05, p <0.01, p <0.001 compared with the OA group. Abbreviations: Con, control; OA, osteoarthritis; BVA, bee venom acupuncture; MA, manual acupuncture; EA, electro-acupuncture; LA, laser acupuncture.
|
Micro-CT imaging revealed that untreated OA knees displayed classic signs of joint degeneration: subchondral erosion, trabecular irregularity, and surface damage (Figure 2). In contrast, the EA, LA, and BVA groups maintained better joint morphology, smoother bone contours, and preserved trabeculae.
 |
Figure 2 Representative micro-CT 3D images. The control knee maintains trabecular subchondral plate integrity with a smooth contour; the OA knee exhibits clear bone erosion following MIA induction. n=8. Abbreviations: Con, control; OA, osteoarthritis; BVA, bee venom acupuncture; MA, manual acupuncture; EA, electro-acupuncture; LA, laser acupuncture.
|
Meniscal ossicles, indicative of OA progression, were significantly enlarged in OA rats (Figure 3). LA significantly reduced ossicle volume and area (p < 0.006 and p < 0.006 vs OA). EA, BVA and MA groups exhibited moderate effects.
 |
Figure 3 Micro-CT analysis of the hind knee joint in MIA-induced OA rats; (A) Area, (B) Volume of the meniscal ossicles. The area and volume of meniscal ossicles, abnormal bone formations within the knee meniscus, across different groups compared to the OA group. Error bars represent standard deviation. p-values indicate significant differences compared to the OA group. n=8. Data are presented as the mean ±standard deviation; p <0.05, p <0.01, p <0.001. Abbreviations: Con, control; OA, osteoarthritis; BVA, bee venom acupuncture; MA, manual acupuncture; EA, electro-acupuncture; LA, laser acupuncture.
|
Safranin-O/Fast Green staining revealed severe cartilage erosion, proteoglycan loss, and chondrocyte disarray in OA rats (Figure 4). EA and LA groups retained matrix staining and structural integrity, similar to the control group. BVA and MA showed partial preservation.
 |
Figure 4 Histological images and quantification of cartilage degradation using Safranin-O/Fast Green staining. (A) Sagittal sections of rat knee joints from each group were stained with Safranin-O/Fast Green. Red staining indicates proteoglycan-rich cartilage, while loss of staining denotes matrix degradation. The OA group showed severe cartilage erosion and proteoglycan loss, whereas the EA and LA groups retained staining patterns similar to the control. Upper row: 10× magnification (scale bars = 100 µm); Lower row: 20× magnification (scale bars = 50 µm). (B) Quantitative assessment of cartilage damage using a modified OARSI scoring system. Boxplots represent median and interquartile range, with individual data points shown. EA and LA groups exhibited significantly lower cartilage scores compared to the OA group (****p < 0.0001, ***p < 0.001, **p < 0.01; one-way ANOVA with Tukey’s post hoc test). Groups with different letters differ significantly, while groups that share a letter do not differ significantly (a-d) (p < 0.05). Abbreviations: Con, control; OA, osteoarthritis; BVA, bee venom acupuncture; MA, manual acupuncture; EA, electro-acupuncture; LA, laser acupuncture.
|
Quantitative scoring confirmed these findings (Figure 4). OA rats had significantly elevated cartilage damage scores (ANOVA, p < 2.2e−16). EA and LA had the lowest scores (p < 0.0001 vs OA), while BVA and MA showed intermediate reductions (p < 0.001, p < 0.01, respectively).
Pain is often the earliest and most persistent symptom of OA, so this study focused on it. We set out to investigate whether EA, LA, and BVA could relieve pain and slow the progression of joint degeneration in MIA-induced OA rats. The results of our study not only confirm the potential of these acupuncture therapies and offer hope and optimism for the future of OA treatment.
Behaviorally, LA and EA improved pain thresholds by Week 2, and by Week 4, LA, EA, and MA significantly reversed mechanical hypersensitivity. Animals in the BVA group experienced some inflammation at the acupoint after treatment; this could account for the low PWT. These effects were verified by micro-CT findings, which showed preserved subchondral structure in EA and LA groups. Rarely assessed in preclinical acupuncture studies, ossicle formation was markedly inhibited by EA and LA, suggesting modulation of aberrant bone remodeling. Safranin-O staining further confirmed that EA and LA most effectively preserved cartilage integrity.
Previous studies have individually validated the efficacy of acupuncture treatments. For instance, Ma et al showed that early EA (at ST35/ST36) preserved cartilage and relieved pain, while delayed EA had reduced benefit.27 Chen et al further revealed that EA acts via sympathetic β2-adrenergic signaling to suppress IL-6, reduce synovial inflammation, and ameliorate pain behaviors.22 Our results align with these findings, as EA improved PWT threshold by week 2 and preserved cartilage, as confirmed by the histology scores.
LA has shown promise in modulating inflammation and promoting cartilage repair.21,28 Li et al demonstrated that 10.6 μm infrared LA reduced MMP-13 expression, improved weight-bearing, and preserved cartilage in MIA-OA rats, resulting in LA’s anti-inflammatory and chondroprotective potential.29 In our study, invasive 830 nm LA produced similar benefits: pain thresholds improved significantly from Week 2, cartilage histology closely resembled that of the control group by Week 4 and reduced ossicle formation. These results suggest that LA, despite being a less invasive and more technologically modern modality, may offer outcomes comparable to EA in treating OA as the LA penetrates deeper into the skin.30
BVA has demonstrated significant analgesic and anti-inflammatory effects through pharmacological mechanisms. Chen and Larivière (2010) reviewed bee venom’s actions and noted its impact on opioid receptors and the suppression of proinflammatory cytokines such as TNF-α and IL-1β.31 Our study supports this mechanistic framework as BVA-treated rats exhibited early pain relief (Week 2) and moderate histological protection. However, its structural preservation was less pronounced than that observed with EA and LA.
A subset of rats in the BVA group developed localized swelling and reduced mobility following the initial bee venom injections. Such responses are consistent with documented side effects of bee venom therapy, which include local inflammation, edema, and, in some cases, systemic reactions. For instance, a systematic review highlighted that bee venom therapy can lead to adverse events ranging from mild local reactions to severe systemic responses, depending on the dosage and administration method. Additionally, studies have reported that bee venom injections can cause localized swelling and pain in animal models. These adverse reactions were not observed in the other treatment groups.32,33
Our findings align with a network meta-analysis by Corbett et al (2013), which found acupuncture among the most effective non-pharmacological treatments for knee OA.16 While their analysis was limited to clinical studies and did not distinguish between acupuncture types, our data add nuance by suggesting that different modalities may yield comparable overall benefits through distinct mechanisms.
Few studies have directly compared EA and LA. Kim et al (2019) evaluated EA and LA in a collagenase-induced arthritis model and reported superior outcomes with LA.20 However, they did not incorporate BVA or assess multiple modalities simultaneously within the same framework. By integrating all three therapies, our study addresses this critical gap and provides clinicians and researchers with comparative evidence to inform integrative treatment strategies.
Understanding how each acupuncture treatment performs could guide therapy selection. Since EA, LA, and BVA function through distinct mechanisms, such as electrical stimulation, PBM, and biochemical immune modulation, understanding their relative effects in one system may inform future combined or personalized protocols. We prioritized functional and structural outcomes over molecular testing to ensure that our findings were closely related to the clinical characteristics of OA.
Acupuncture reduced both pain behaviors and cartilage degeneration in MIA-induced KOA, but the benefit was contingent upon the specific modality employed. LA had the most substantial and persistent therapeutic results, as indicated by changes in pain thresholds, cartilage, and bone structure. Its effectiveness outperformed that of EA and MA. In contrast, BVA had little efficacy and caused acute adverse reactions. This study suggests that the therapeutic efficacy of acupuncture for KOA is determined by the modality used, with laser-based approaches outperforming other methods. These findings emphasize the potential for adapting acupuncture modalities to disease pathophysiology and the importance of integrative, comparative research in advancing complementary OA therapies.
BVA, bee venom acupuncture; CT, computed tomography; EA, electroacupuncture; EDTA, ethylenediaminetetraacetic acid; GB34, gall bladder 34 acupoint (yanglingquan); LA, laser acupuncture, MA, manual acupuncture; MIA, monosodium iodoacetate; OA, osteoarthritis; PWT, paw withdrawal threshold; PBM, photobiomodulation.
The data generated for the present study are available from the corresponding author, Gihyun Lee: [email protected], and Jae-Hong Kim: [email protected], upon reasonable request.
This study was approved by the animal care and use committee of Dongshin University (DSU-2024-07-04).
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: RS-2023-KH139215).
The authors declare that they have no conflicts of interest in this work.
1. David J, Hunter P, Sita Bierma-Zeinstra P. Osteoarthritis. Lancet. 2019;1745–1759.
2. Safiri S, Kolahi -A-A, Smith E, et al. Global, regional and national burden of osteoarthritis 1990-2017: a systematic analysis of the global burden of disease study 2017. Ann Rheumatic Dis. 2020;79(6):819–828. doi:10.1136/annrheumdis-2019-216515
3. Conaghan PG, Dickson J, Grant RL. Care and management of osteoarthritis in adults: summary of NICE guidance. BMJ. 2008;336(7642):502–503. doi:10.1136/bmj.39490.608009.AD
4. O’Neil CK, Hanlon JT, Marcum ZA. Adverse effects of analgesics commonly used by older adults with osteoarthritis: focus on non-opioid and opioid analgesics. Am J Geriatric Pharmacother. 2012;10(6):331–342. doi:10.1016/j.amjopharm.2012.09.004
5. Janusz M, Hookfin E, Heitmeyer S, et al. Moderation of iodoacetate-induced experimental osteoarthritis in rats by matrix metalloproteinase inhibitors. Osteoarthritis Cartilage. 2001;9(8):751–760. doi:10.1053/joca.2001.0472
6. Guingamp C, Gegout‐Pottie P, Philippe L, Terlain B, Netter P, Gillet P. Mono‐iodoacetate‐induced experimental osteoarthritis. A dose‐response study of loss of mobility, morphology, and biochemistry. Arthritis Rheum. 1997;40(9):1670–1679. doi:10.1002/art.1780400917
7. Han J-S. Acupuncture and endorphins. Neurosci Lett. 2004;361(1–3):258–261. doi:10.1016/j.neulet.2003.12.019
8. Kamau V, Lee G, Kim JH. Therapeutic effects of invasive laser acupuncture at GB34 on monosodium iodoacetate-induced osteoarthritis rats. Osteoarthritis Cartilage. 2025;33:S477. doi:10.1016/j.joca.2025.02.697
9. Chen S, Zhang GY, Wang YY, et al. Effect of moxibustion and scraping on bioactive substances of acupoints in knee osteoarthritis rats. Zhen Ci Yan Jiu. 2023;48(4):359–365. doi:10.13702/j.1000-0607.20220994
10. Lee J-H, Choi T-Y, Lee MS, Lee H, Shin B-C, Lee H. Acupuncture for acute low back pain: a systematic review. Clin J Pain. 2013;29(2):172–185. doi:10.1097/AJP.0b013e31824909f9
11. Lee H-S, Park J-B, Seo J-C, Park H-J, Lee H-J. Standards for reporting interventions in controlled trials of acupuncture: the STRICTA recommendations. J Acupuncture Res. 2002;19(6):134–154.
12. MacPherson H, White A, Cummings M, et al. Standards for reporting interventions in controlled trials of acupuncture: the STRICTA recommendations. Acupuncture Med. 2002;20(1):22–25. doi:10.1136/aim.20.1.22
13. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American college of rheumatology/arthritis foundation guideline for the management of osteoarthritis of the hand, Hip, and knee. Arthritis Rheumatol. 2020;72(2):220–233. doi:10.1002/art.41142
14. Manheimer E, Linde K, Lao L, Bouter LM, Berman BM. Meta-analysis: acupuncture for osteoarthritis of the knee. Ann Internal Med. 2007;146(12):868–877. doi:10.7326/0003-4819-146-12-200706190-00008
15. Manheimer E, Cheng K, Linde K, et al. Acupuncture for peripheral joint osteoarthritis. Cochrane Database Syst Rev. 2010;2010(1). doi:10.1002/14651858.CD001977.pub2
16. Corbett M, Rice S, Madurasinghe V, et al. Acupuncture and other physical treatments for the relief of pain due to osteoarthritis of the knee: network meta-analysis. Osteoarthritis Cartilage. 2013;21(9):1290–1298. doi:10.1016/j.joca.2013.05.007
17. Chen J, Liu A, Zhou Q, et al. Acupuncture for the treatment of knee osteoarthritis: an overview of systematic reviews. Int J Gene Med. 2021;Volume 14:8481–8494. doi:10.2147/IJGM.S342435
18. Lee J-D, Park H-J, Chae Y, Lim S. An overview of bee venom acupuncture in the treatment of arthritis. Evidence-Based Complementary Alternative Med. 2005;2(1):79–84. doi:10.1093/ecam/neh070
19. Cherniack EP, Govorushko S. To bee or not to bee: the potential efficacy and safety of bee venom acupuncture in humans. Toxicon. 2018;154:74–78. doi:10.1016/j.toxicon.2018.09.013
20. Kim M, Lee Y, Choi D, Youn D, Na C. Effects of laser and electro acupuncture treatment with GB30· GB34 on change in arthritis rat. Korean J Acupuncture. 2019;36(4):189–199. doi:10.14406/acu.2019.023
21. Law D, McDonough S, Bleakley C, Baxter GD, Tumilty S. Laser acupuncture for treating musculoskeletal pain: a systematic review with meta-analysis. J Acupuncture Meridian Studies. 2015;8(1):2–16. doi:10.1016/j.jams.2014.06.015
22. Chen W, Zhang X-N, Su Y-S, et al. Electroacupuncture activated local sympathetic noradrenergic signaling to relieve synovitis and referred pain behaviors in knee osteoarthritis rats. Front Mol Neurosci. 2023;16:1069965. doi:10.3389/fnmol.2023.1069965
23. Zhang W, Zhang L, Yang S, Wen B, Chen J, Chang J. Electroacupuncture ameliorates knee osteoarthritis in rats via inhibiting NLRP3 inflammasome and reducing pyroptosis. Mol Pain. 2023;19:17448069221147792. doi:10.1177/17448069221147792
24. Ro JY, Zhang Y, Tricou C, Yang D, da Silva JT, Zhang R. Age and sex differences in acute and osteoarthritis-like pain responses in rats. J Gerontol Ser A. 2020;75(8):1465–1472.
25. Tan Q, Cai Z, Li J, et al. Imaging study on acupuncture inhibiting inflammation and bone destruction in knee osteoarthritis induced by monosodium iodoacetate in rat model. J Pain Res. 2022;Volume 15:93–103. doi:10.2147/JPR.S346242
26. Bove S, Calcaterra S, Brooker R, et al. Weight bearing as a measure of disease progression and efficacy of anti-inflammatory compounds in a model of monosodium iodoacetate-induced osteoarthritis. Osteoarthritis Cartilage. 2003;11(11):821–830. doi:10.1016/S1063-4584(03)00163-8
27. Ma Y, Guo H, Bai F, et al. A rat model of knee osteoarthritis suitable for electroacupuncture study. Experimental animals. 2018;67(2):271–280. doi:10.1538/expanim.17-0142
28. Kim J-H, Na C-S, Cho M-R, Park G-C, Lee J-S. Efficacy of invasive laser acupuncture in treating chronic non-specific low back pain: a randomized controlled trial. PLoS One. 2022;17(5):e0269282. doi:10.1371/journal.pone.0269282
29. Li Y, Wu F, Wei J, Lao L, Shen X. The effects of laser moxibustion on knee osteoarthritis pain in rats. Photobiomodul Photomed Laser Surg. 2020;38(1):43–50. doi:10.1089/photob.2019.4716
30. Chon TY, Mallory MJ, Yang J, Bublitz SE, Do A, Dorsher PT. Laser acupuncture: a concise review. Med Acupuncture. 2019;31(3):164–168. doi:10.1089/acu.2019.1343
31. Chen J, Lariviere WR. The nociceptive and anti-nociceptive effects of bee venom injection and therapy: a double-edged sword. Progress Neurobiol. 2010;92(2):151–183. doi:10.1016/j.pneurobio.2010.06.006
32. Kwon Y-B, Lee J-D, Lee H-J, et al. Bee venom injection into an acupuncture point reduces arthritis associated edema and nociceptive responses. Pain. 2001;90(3):271–280. doi:10.1016/S0304-3959(00)00412-7
33. Lee JA, Son MJ, Choi J, Jun JH, Kim J-I, Lee MS. Bee venom acupuncture for rheumatoid arthritis: a systematic review of randomised clinical trials. BMJ open. 2014;4(11):e006140. doi:10.1136/bmjopen-2014-006140
Chronic pain is a significant global health burden.1 The impact of persistent pain on patients’ social engagement is considerable, often resulting in reduced participation or avoidance of daily and social activities due to the…
